Dr. Kyriazis is one of Britain’s top anti-aging physicians and is internationally recognised as a pioneer in the field. He is a bio-gerontologist with a medical degree and postgraduate degrees from King’s College, London and the Royal College of Physicians. He has written many books for both the medical professional and the public alike and his articles have been widely published. In 1991 Dr. Kyriazis founded the British Longevity Society, one of the earliest societies in the field still operating today.
Dr. Marios Kyriazis brings a wealth of medical expertise to one of the most important breakthroughs in recent times to help combat a disease called ‘senile cataract,’ a disease that affects one in five people over the age of 55.
In the past, the only treatment available for this chronic condition was surgery, which by its very nature can lead to serious complications. We must also consider that the replacement of a natural lens with a plastic one leads to a loss in accommodation; in brief a plastic lens is not as good as a natural one.
But now other non-surgical treatments are available, in particular the Russian development of N-acetyl-carnosine. In clinical trials this eye-drop treatment has shown dramatic and impressive results in treating age related cataracts.
Furthermore, The Cataract Cure also covers other associated eye disorders including;
The Cataract Cure is a resource for all persons interested in knowing about alternative approaches to eye care, approaches that are still proven, scientific and based in clinical experience.
Disclaimer
The information contained within this book is based on the experience and research of the author. It is not intended to substitute for a medical consultation and any attempt to diagnose or treat a disease should only be done under the guidance of a medical professional.
The publisher does not advocate the use of any particular protocol, but believes the information should be made available to the public. The publisher therefore cannot be responsible for any adverse effects or consequences arising from the use of any suggestions or procedures that are discussed in this book.
Any decision made in purchasing goods and/ or services as a result of information obtained within is your sole responsibility. We will not be liable to any customer for any information supplied in this publication and it is provided on an ‘as is’ basis.
Should the reader have any questions concerning the preparations or procedures mentioned herein, the publisher strongly recommends consulting with a professional health care advisor.
Copyright 2010
All rights are reserved, no part of this publication may be used or reproduced by an means, graphic, electronic or mechanical, including photocopying, recording, taping or by any information storage retrieval system without the written permission of the publisher- except in the case of brief quotation embodied in critical articles and reviews.
IAS, PO Box 19, Sark GY9 0SB, Great Britain
Contents
o By Phil Micans, MS, PharmB
o Carnosine
o Metformin
o Aminoguanidine
o Melatonin
o Cataracts
o Glaucoma
o Macular degeneration
o Background
o Issues
o Nutrients
o Lipid peroxidation
o Activity and properties
o Research
o Photographs
o Other indications
o FAQs
o Case studies
o Testimonials
o Conclusion
o Glossary
o Suppliers
o References
o Websites
o Biography
o Reviews
Foreword
As a researcher my work has taken me around the globe in search of new and exciting developments in the hunt for both preventative and curative therapies.
The world has many innovative products and technologies that are not well known and from time to time a particularly exciting development come to the fore; N-acetyl-carnosine eye-drops for cataract are just such an example.
In this publication Dr. Kyriazis highlights the background to its development and its studies and also looks at the clinical applications that make these eye-drops special. In addition, his patient examples and testimonials bring that intimate feeling that makes a discovery something personal and somehow even more important.
With an ever increasing ‘older’ population the incidences of age-related disorders such as senile cataract are ever more prevalent. As Dr. Kyriazis highlights in ‘The Cataract Cure’ this new research has proven that an eye-drop can slow, arrest and even reverse cataracts. Therefore, it not only represents an excellent example of ‘antiaging medicine’ at its best, it is also an important breakthrough for eye care.
Dr. Kyriazis book doesn’t ‘just’ discuss the topic of cataracts, but includes additional information regarding other class leading therapies and nutrition; procedures that can ameliorate and improve many other troubling eye-sight problems including glaucoma and macular degeneration.
My recommendation is that anyone who is concerned about their failing eyesight and vision difficulties should digest and act upon the information presented here.
Phil Micans, MS, PharmB
——————————————————————————–
Chapter 1: Introduction
History tells us that we now live longer than ever before. Scientific advances have ensured that many illnesses have been successfully eliminated and newer therapies are being discovered to deal with existing illnesses. Within the next 20 years we may experience an even more dramatic extension of the human life-span, made possible by discoveries in the field of genetics, stem cells, growth factors, calorie restriction mimetics and nanotechnology. Until that moment arrives, we need to deal with existing age-related disorders as best we can, and to be able to do this, we need to know exactly how aging works.
Most anti-aging researchers and physicians accept that a major factor involved in aging is damage caused by free radicals. These are a group of simple compounds with an electron missing form their chemicals structure. The lack of electron makes free radicals very unstable. Due to reasons based on chemistry and chemical laws, free radicals need to obtain the missing electron from somewhere, and so they must seek out other molecules from which they can acquire an electron.
Examples of free radicals are:
These reactive molecules destroy other molecules around them causing what we now call ‘aging’. Free radicals affect every organ of your body, constantly. By the time you have finished reading this sentence, your DNA, proteins and cells have already been, minutely but irreversibly, damaged.
Therefore, it is important to keep free radicals under control, and Nature has made arrangements for this. We carry inside us a variety of antioxidants, natural chemicals which mop up free radicals and destroy them, keeping damage low. The problem is, with the passage of time, the effectiveness of these antioxidants worsens, and so we become unable to fight free radicals effectively. In this way, age-related damage accumulates until the time of death.
Apart from free radicals, another important cause of aging is glycation. During everyday metabolism, natural chemicals in your body such as glucose, fructose, aldehydes and ketones may attach themselves onto your proteins, during a process called glycation. This reaction is also sometimes called the Maillard reaction. It results in a glycated protein, i.e. a protein carrying sugar (or similar) molecules on it. This glycated protein may then react with any other proteins resulting in irreversible bonding between the two. This bonding process is named ‘cross-linking.’
Affected molecules can be anything from collagen and elastin (found in your skin, arteries or other internal tissues), to enzymes and proteins of the immune system. Facilitators during the cross-linking process are the carbonyl groups which act like glue, fixing the two proteins together. Carbonyls are fragments of chemicals which are formed as a result of a sugar (or an aldehyde or a ketone or a free radical) reacting with amino acids on a protein. Also, carbonyls can be formed in other situations involving fats or DNA. So, carbonyls may not only cause protein-to-protein cross-linking, but also protein-to-DNA, or protein-to-lipid cross-linking, which is equally damaging to your body.
Cross-linking results in formation of large insoluble amounts of damaged proteins in the tissues, including the eye. These damaged proteins are called AGEs (Advanced Glycation End products) and may then go on to combine with free radicals and cause yet more tissue injury (this is called ‘chronic oxidation’). Although a steady rate of AGE formation happens as a result of normal aging (starting after the age of 20), formation of AGEs is accelerated during diabetes. AGEs then block activities within the cells, stimulate cells to produce more free radicals (such as superoxide and nitric oxide), and activate toxic chemical such as Tumour Necrosis Factor alpha (TNF-a) and interleukin 6. In this way, AGEs are contributing to age-related chronic diseases or even cancer.
Chronic diseases which can be caused by glycation and cross-linking are:
There are commercially available blockers of cross-linking (antiglycators). Examples of these include carnosine, aminoguanidine, metformin, acarbose, and pyridoxamine. Some of these (like acarbose and metformin) are already in use as drugs against diabetes, but new research coming to light is now emphasising their additional anti-cross-linking effects. However, only carnosine (under the form of N-acetylcarnosine) can be given in eye drops form for treatment of chronic eye conditions.
Three examples of effective anti-glycators are:
1. Carnosine
This combination of the amino acids beta alanine and L-histidine is a naturally-occurring agent found in muscle and nervous tissue. Carnosine has been hailed as one of the most promising cross-link inhibitors, and so it has been used against cataract as you will soon see. It has multiple actions and as such it has been called a pluripotent agent. One way carnosine works is by scavenging for free carbonyl groups. It is one of the few cross-link inhibitors thatis not only active against protein-to-protein cross-linking but also against protein-to-DNA cross-linking.
Carnosine has a direct antioxidant action, and it also protects and activates many other antioxidants, such as glutathione. It is a strong chelator of heavy metals, mopping-up any toxic metal ions in your body which may result in accelerated free radical attack. Finally, it has a possible, yet unconfirmed, bond-breaking capability by dissolving certain bonds (S-S bonds) on cross-linked proteins. In measurements of arterial wall flexibility, carnosine seems to be able to relax the arterial wall and thus improve blood flow. This particular benefit of carnosine may be related to its ability to stimulate nitric oxide, a molecule that relaxes the muscles within the arteries.
Several experiments have highlighted carnosine’s ability to reduce free radical and glycation metabolism, both in humans and in animals. One of the most important developments regarding carnosine is its ability to prevent and cure age-related cataract, and possibly glaucoma and other chronic eye conditions. In this respect the form of carnosine used is N-acetylcarnosine. This curative action of carnosine is perhaps related to its ability to stimulate elimination of damaged proteins from the eye.
The dose of oral carnosine is anything from 50 mg to 300 mg a day, up to 500 mg to 1500 mg a day. With higher doses, there have been occasional reports of allergic reactions. Carnosine can also be obtained from a meat rich diet, particularly from chicken breast, rabbit, pheasant and other game (especially sprinting animals).
The interest in the use of carnosine and its derivatives for the treatment of cataract has been increasing over the past 3 years. Writing for a major peer-review journal, scientists from the Department of Ophthalmology, Christchurch Hospital, Christchurch New Zealand, have commented: “Since the last major review of medical treatment of cataract the search for an anti-cataract agent has advanced on many fronts. Some anti-cataract drugs, such as carnosine, have now reached clinical trials and showed encouraging results that warrant further investigation. The discovery of an effective medical treatment for cataract is likely to make global impact on eye health.”
Reference: Toh T, Morton J, Coxon J, Elder MJ. Medical treatment of cataract. Clin Experiment Ophthalmol. 2007;35(7):664-71.
2. Metformin
Metformin is a frequently used drug used against diabetes (both against the insulin-dependent and against the non-insulin-dependent varieties). It can also lower cholesterol, reduce body fat, beef-up antioxidant defences and inhibit glycation. It limits the formation of AGEs, particularly those affecting collagen.
Recent experiments show metformin to have widespread activities as a cross-link inhibitor. It reduces cross-linking of fibrin proteins which take part in the clotting of blood. Exaggerated cross-linking of fibrin results in abnormal blood clotting and therefore an increased risk of thrombosis with consequent heart disease or stroke.
There are no clinical studies evaluating metformin in cataract, but diabetic patients who are already on it are likely to be receiving its antioxidant, antiglycating benefits. Moreover, because it helps improve the circulation of the blood (by reducing the risk of thrombosis), it may be additionally useful in eye diseases such as macular degeneration, cataract and glaucoma.
Metformin is a calorie restriction mimetic which means it has many biological benefits associated with calorie restriction itself. Calorie restriction is the only proven method that can increase maximum lifespan, and reduces the likelihood of age-related conditions, including cataract.
3. Aminoguanidine
An agent structurally similar to metformin is aminoguanidine. As with the case of metformin, aminoguanidine also works by reducing the concentration of free carbonyl groups. In particular, it is active against certain aldehydes which contribute to cross-linking. It is effective mainly during the early stages of glycation.
Aminoguanidine is a potent inhibitor of any cross-linking which is initiated by glucose molecules but not as effective in situations involving ribose-related cross-linking. In any case, it prevents collagen cross-linking in tendons and skin, which shows its potential for prevention of muscle and joint age-related stiffness, and skin ageing (wrinkles). It limits the development of diabetic complications in animals (including eye complications), and it has shown promising effects in improving diabetic kidney disease. Also, it is a weak copper chelator. Copper chelation is important in AGE-induced damage, as high amounts of free copper are more likely to increase AGE-induced injury.
An additional action of aminoguanidine is that it prevents cross-linking between lipoproteins (proteins carrying fat molecules) and therefore reduces the risk of blockage of the arteries, particularly the small arteries that feed the small nerves of the eye. It should, therefore, be of use in eye conditions were blood supply is compromised. Experiments using aminoguanidine in eye drops form for prevention of cataract are currently under way.
Apart from anti-glycators, certain other agents have specific and promising benefits on eye disease. One such agent is melatonin.
Melatonin in some age-related eye conditions
In the eye, melatonin is produced in the retina, but production gradually declines with age. Adding extra oral melatonin supplements is believed to protect against many degenerative eye conditions. The presence of cell receptors for melatonin in the eye indicates that this substance has an important physiological role to play in several functions related to vision.
It has been shown that melatonin (N-acetyl-5-methoxytryptamine) prevents free radical damage to the tissues and also it scavenges and neutralises free radical in the eye.
Current evidence suggests that melatonin may protect against eye diseases such as cataract, keratitis, glaucoma, retinopathy and other injury to the eye. The cause of these conditions is thought to be, partly, due to oxidation damage which causes loss of cells (apoptosis), and degeneration of retinal neurons. Free radicals such as nitric oxide in the eye neurons and superoxide in the mitochondria of the axons produce dangerous toxins such as peroxynitrite. Among the substances that have actions against peroxynitrite is also melatonin.
Also see the paragraph below for further information of melatonin in the treatment of macular degeneration.
Cataract
In cancer patients undergoing radiotherapy, the effect of irradiation on the eye can be significant, contributing to a worsening of cataract. However, researchers from the Department of Radiation Oncology, Atatürk University, in Turkey have shown that melatonin supplements protect the lens of the eyes from radiation-induced cataract formation. The researchers suggest that supplementing cancer patients with melatonin may reduce the risk of radiotherapy-induced tissue injury.
Glaucoma
With regards to glaucoma, current research suggests that it could reduce intraocular pressure and so it can be of real help in this condition.
Reference: Mediero A, Alarma-Estrany P, Pintor J. New treatments for ocular hypertension. Auton Neurosci. 2009 11;147(1-2):14-9.
Note- this is believed to be due to melatonin’s antioxidant effect, which is still being investigated.
Macular degeneration
Researchers from the Zhongshan Ophthalmic Center, Sun Yat-Sen University in China have reported that melatonin can help reduce the progression of macular degeneration. It is well known that melatonin controls eye pigmentation and so regulates the amount of light that reaches the visual receptors in the eye.
These researchers studied 100 patients suffering from either the wet or the dry form of macular degeneration. The patients were given 3 mg of melatonin every night, (the precise formula was designed by Dr. Walter Pierpaoli and also contained zinc and selenium in addition to the melatonin, it is called Melatonin Zn-Se or MZS™).
After a six month period, the scientists found that the patients’ visual acuity was stable, i.e. there was a slowing down of the natural worsening of the condition. The scientists said: “We conclude that the daily use of 3 mg melatonin [with zinc and selenium] seems to protect the retina and to delay macular degeneration. No significant side effects were observed. “
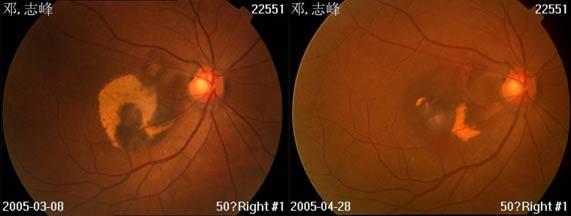
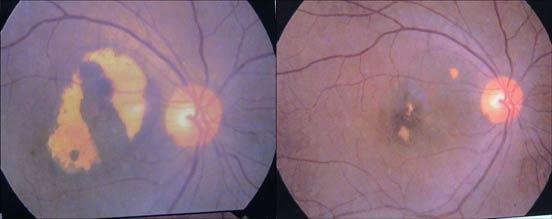
These photographs (fundus pictures) attest to the slowing and reversal of both wet and dry forms of age related macular degeneration (ARMD). Patients took one MZS™ tablet (3mg melatonin, 50mg zinc and 50mcg selenium) nightly.
Top set: The left slide shows the eye of a 67 year old male before treatment, his vision had been deteriorating for 2-years. The right picture shows the same eye 2-months later after daily ingestion of one MZS™ tablet nightly. He now has stable visual acuity of 0.3 with remarkable improvements in sub-retinal macular hemorrhage.
Bottom set: The left slide shows the eye of a 71-year old female with ARMD before treatment. The right slide is her eye after 6-months of one MZS™ tablet nightly. Her vision improved from 0.2 to 0.4 (as indicated in the right slide).
Reference: Effects of melatonin in age related macular degeneration. Changxian Yi, Xiaoyan Pan, Hong Yan, Mengxiang Guo, Walter Pierpaoli. New York Academy of Science, volume 1057, 385-392, December 2005.
A recent report by Austrian scientists confirms the antioxidant properties of melatonin with regards to the eye, commenting that patients with macular degeneration try to produce more melatonin as a defence mechanism against the condition.
Reference: Schmid-Kubista KE, Glittenberg CG, et al. Daytime levels of melatonin in patients with age-related macular degeneration. Acta Ophthalmol. 2009;87(1):89-93.
So, to summarise, free radicals and glycation are two important causes of aging, and can cause a variety of chronic diseases, including cataract and other degenerative eye diseases. Certain nutrients and drugs are now commercially available, which may help protect against such chronic diseases.
Chapter 2: Cataract
Age-related (senile) cataract is a chronic, progressive eye disease affecting the lens in the eye, resulting in reduced vision. The lens is a transparent, pale yellow structure made of special proteins (crystallins) and other clear material, allowing the light to pass through and focus onto the retina, so an image can be formed. It is found behind the pupil of the eye and it is surrounded by an elastic capsule. The lens is a relatively simple structure and it grows throughout life from the inside outwards.
When the lens is affected by age-related damage, it becomes opaque and cloudy, reducing the amount of light reaching the inside of the eye and so vision is impaired.
Did you know?
Cataract is a Greek world, meaning ‘waterfall’. Indeed, the ancient Greeks compared the visual impairment of a patient with cataract to the difficulties in trying to see through a waterfall.
Cataract affects one in four people over the age of 65, and one in two people aged 80 and above. About 28 000 new cases worldwide are reported every single day, and 17 million people across the world are blind due to cataract. Operations to treat cataract cost the US alone $3.5 billion a year, and 43% of visits to eye specialists in the United States are associated with cataract. Therefore, there is considerable interest in finding ways to prevent the condition and reduce the burden upon health-providers.
The problem is that in developing countries cataract remains, on the whole, untreated due to lack of resources. In such countries it is a major cause of blindness. It is impossible to provide enough eye surgeons to manage all the cases of cataract in developing countries, not only due to the high cost involved but also due to lack of manpower.
Did you know?
Around 9 million people in developing countries (in Africa and Asia) are blind due to cataract. Put another way, one in every hundred residents of Africa is blind, and the frequency of the disease is increasing.
As we generally live longer than ever before, age-related diseases such as cataract are now becoming more frequent and affect people for longer. However, cataract does not only happen to older people. Younger groups are also affected. Apart from genetic causes of cataract, two well known causes are use of steroids and diabetes. Also, diet has been implicated as a cause. People who consume poor quality food are at a greater risk of cataract, and poverty is a risk factor making cataract more likely. This may be because a diet which is poor in high quality vegetables, protein and fruit does not provide enough nutrients to prevent the free radical damage to the eye.
You may remember from the discussion in Chapter 1 that free radicals and glycation cause proteins inside the lens to attach to each other, a process called cross-linking. This mass of abnormal proteins scatters the light and does not allow it to pass through. The crystallins in the lens become abnormally distorted and can settle in different parts of the lens, for example the top, the middle, the outside, or the entire lens, causing different types of cataract. What is important here is that an opaque lens is not a useful lens, as the light must pass through it uninterrupted. Therefore, any treatment which reduces damage to crystallins is bound to result in effective clinical improvement of cataract.
From the nutritional point of view, lack of antioxidants in the diet has been shown to worsen the risk of cataract and other eye diseases such as glaucoma. Patients with cataract are frequently found to be deficient in antioxidants such as vitamin A, glutathione, lutein and zeaxant